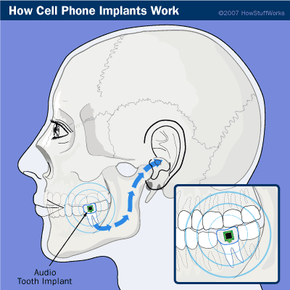
In November 2002, designers at the Royal College of Art in London made headlines after coming up with the world's first cell-phone implant. Their design involved a small chip that housed a receiver and a transducer. The receiver could pick up mobile phone signals, and the transducer could translate them into vibrations.
Once implanted in a person's molar, the transducer caused the tooth to vibrate in response to radio signals. The physical structure of the jaw carried the tooth's vibrations to the inner ear, where the user, and no one else, could perceive them as sound. The implant's designers held dramatic demonstrations of this principle using a vibrating wand. Participants confirmed that they could hear crystal clear voices through their teeth.
Advertisement
The designers used a wand for the demonstrations rather than the implant itself because the implant did not actually exist. It was a concept, not a real device. In addition, it wasn't really a phone -- it was more like one of the Bluetooth earpieces commonly used today. It had no mechanisms for dialing, storing phone numbers or anything else that a phone can do, other than relaying sounds to the listener. The theoretical implant's design didn't even allow the user to speak to the party on the other end of the line.
Even though it wasn't actually a working phone, the Royal College of Art project got people thinking about implantable phone technology. Cell phones have gotten a lot smaller since they hit the market, so one that is small enough to fit inside a person seems inevitable. The recent preponderance of tiny, functional Bluetooth earpieces has also made the idea of a discreet, permanent implant seem viable to a lot of people.


But even though they're a lot smaller than they used to be, modern cell phones are still far too big to fit inside your body. Even the smallest Bluetooth earpieces are really too big to fit anywhere other than your abdomen or chest. In either of these locations, a cell phone would be impractical, inconvenient and dangerous. Implanting one would require major surgical procedures under general anesthesia.
For these reasons, developers had to make numerous modifications to existing cell phone designs to create a complete, working cell-phone implant. Rather than using a single piece inserted under a person's skin, cell-phone implants are modular in design. Implantation requires several small, separate incisions and local anesthetic. The different pieces communicate with each other using flexible circuitry and conductive tattoo ink, and each piece is specially designed to be as small and comfortable as possible.
In this article, we'll look at all the parts of the cell-phone implant and how they communicate with each other. We'll also examine the pros and cons of making your phone part of your body.
Advertisement